
Zelboraf is indicated for the treatment of metastatic melanoma and Erdheim-Chester disease.
The drug was developed by Plexxikon in collaboration with Roche. Plexxikon was acquired by Daiichi Sankyo in April 2011.
Recommended Buyers Guides
Zelboraf is marketed by Genentech in the US. The biotechnology corporation submitted a new drug application (NDA) to the US Food and Drug Administration (FDA) for the drug in May 2011. It was reviewed under fast-track designation and approved for use in patients with metastatic melanoma in August 2011.
The FDA’s approval was based on the results of Phase II trial BRIM2 and Phase III study BRIM3.
In 2017, the FDA expanded the drug’s label to treat patients with Erdheim-Chester disease with BRAF V600 mutation.
A marketing authorisation application (MAA) was submitted to the European Medicines Agency (EMA) in May 2011. The EC approved the drug in February 2012.
The drug is approved in Canada, Switzerland, Brazil, Israel, Mexico, Australia and New Zealand.
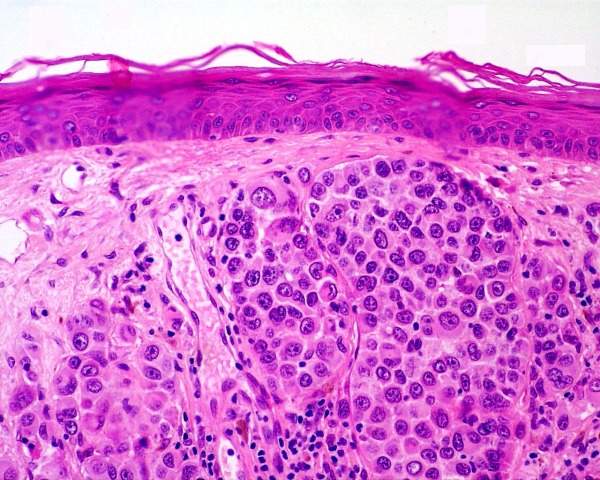
Treatment for advanced skin cancer metastatic melanoma
Melanoma is a type of skin cancer that forms in the melanocyte cells, which are responsible for the skin’s colour.
The disease can be treated in its early stages, but it spreads to other parts of the body with time, causing metastatic melanoma, an aggressive and advanced-stage skin cancer.
Metastatic melanoma patients have low life expectancy. Symptoms include loss of appetite, nausea, vomiting and fatigue. Spread of cancer to the brain (brain metastases) is common in these patients.
Around 160,000 patients worldwide are diagnosed with Melanoma every year.
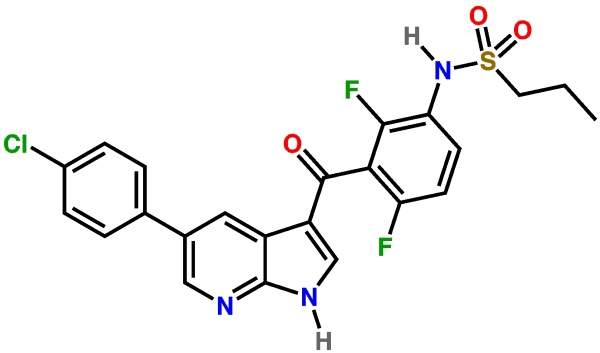
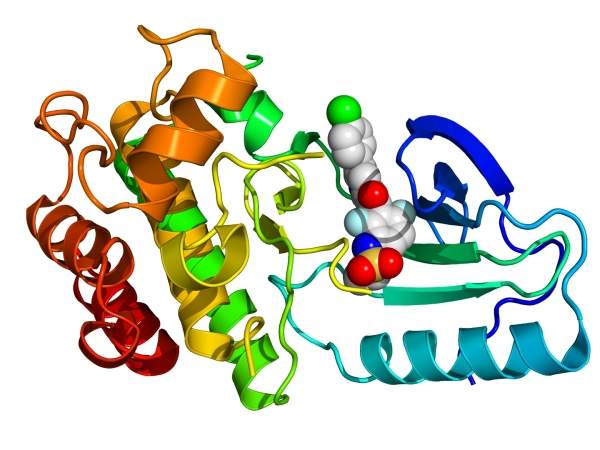
Zelboraf’s mechanism of action
Cells require the BRAF protein to grow. Mutations in these proteins may cause the protein to not ‘switch off’, resulting in constant growth signals. These signals lead to cancer development and growth.
Zelboraf was designed using the cobas 4800 BRAF V600 mutation diagnostic test. The drug inhibits the mutant forms of BRAF protein to prevent cell growth and cancer development.
Phase I and II clinical trials of Zelboraf
Plexxikon jointly conducted Phase I, II and III trials with Roche as part of a deal that was signed in 2006.
Phase I trial data was released in June 2009. Around 55 melanoma patients were enrolled, which included 24 people that had mutated BRAF mutant proteins. Trial data from 16 BRAF-positive melanoma patients showed the drug was tolerable.
A tumour regression of 30% was achieved in nine of the patients. The median progression-free survival (PFS) was seven months, while around 20% developed squamous cell carcinoma.
Phase II trial BRIM2 was conducted on 132 patients that had received prior treatment for BRAF V600 mutation positive metastatic melanoma. Initiated in September 2009, the trial’s data was released in November 2010.
The primary endpoint was to achieve overall response rate (ORR). Tumour shrinkage was observed in around 53% of patients at a median time of 6.7 months. Overall survival (OS) was not achieved after a ten-month follow-up. The side effects observed included joint pain, rashes, sensitivity to sun and fatigue.
In January 2011, a Phase I trial was initiated to evaluate the effect of food on the pharmacokinetics of a single dose of vemurafenib. They were then administered twice daily doses until disease progression or until toxicity was observed.
Around 132 patients were enrolled in a Phase II trial to evaluate the safety and efficacy of the drug in melanoma patients with brain metastases. The trial was initiated in July 2011 and is scheduled to be completed by September 2012. Patients were administered 960mg of vemurafenib twice daily until disease progression, toxicity or consent withdrawal.
In September 2011, a Phase I/II trial was initiated in 50 patients with BRAF V600 positive metastatic melanoma. The trial was conducted to evaluate the safety and efficacy of the drug, as well as to determine the anti-cancer effects and survival rate of patients treated with Vemurafenib in combination with ipilimumab.
Phase III clinical trials of Zelboraf
A Phase III trial named BRIM3 was initiated in January 2010. Around 675 patients with previously untreated BRAF V600 mutation-positive melanoma were enrolled. The primary endpoint was OS rates and PFS.
Trial data released in June 2011 showed around 63% of the patients had lower risk of worsening the disease compared to that of patients given chemotherapy.
The response rate in patients treated with vemurafenib was nine times higher than in those treated with chemotherapy. Around 84% of the patients survived after six months of treatment, compared to 64% in case of chemotherapy.
The FDA’s approval of the drug for Erdheim-Chester disease was based on the positive outcomes of an open-label, multi-centre, single-arm, multiple cohort clinical trial that enrolled 22 patients with BRAF V600 mutation- positive Erdheim-Chester disease, aged 16 years or older.
The overall response rate was 54.5%. Around 50% of patients observed partial response and 4.5% observed complete response during the trial.