In the US, the disease burden of type 2 diabetes is marked by stark racial inequities. Extensive literature has noted that racial minorities have shown higher prevalence rates of type 2 diabetes, a pattern frequently attributed to greater exposure to socioeconomic and environmental cardiometabolic risk factors. However, little scholarship has explored the racial dynamics of type 2 diabetes treatment.
In a recent publication in The Lancet Regional Health – Americas, Rodriguez and colleagues observed the degrees of type 2 diabetes treatment using sodium-glucose cotransporter 2 inhibitors (sGLT2is) or glucagon-like peptide-1 receptor agonists (GLP-1 RAs) among various races and ethnicities. GlobalData epidemiologists forecast an increase in the diagnosed prevalent cases of type 2 diabetes from more than 23,260,000 to almost 24,582,000 cases between 2024 and 2028. Amidst the urgent rise in type 2 diabetes cases in the US, Rodriguez and colleagues’ study brings further attention to racial disparities behind this broader epidemiological trend.
Go deeper with GlobalData


Access deeper industry intelligence
Experience unmatched clarity with a single platform that combines unique data, AI, and human expertise.
In a retrospective cohort study, Rodriguez and colleagues observed six nationally representative electronic health record registries between 2014 and 2022. Their analysis, which covered more than 687,000 adult patients, segmented patients by their race and ethnicity, with the main endpoint being the dispensation of at least one sGLT2i or GLP-1 RA medication for diabetes in a year. The authors also measured HbA1c levels and cardiometabolic comorbidity prevalence. The study cohort exhibited growth in the dispensing of both sGLT2i and GLP-1 RAs, showing an uptake of 0.1% to 12.2% and 0.3% to 3.4%, respectively, across the study period.
Disease management marred by limited access to care
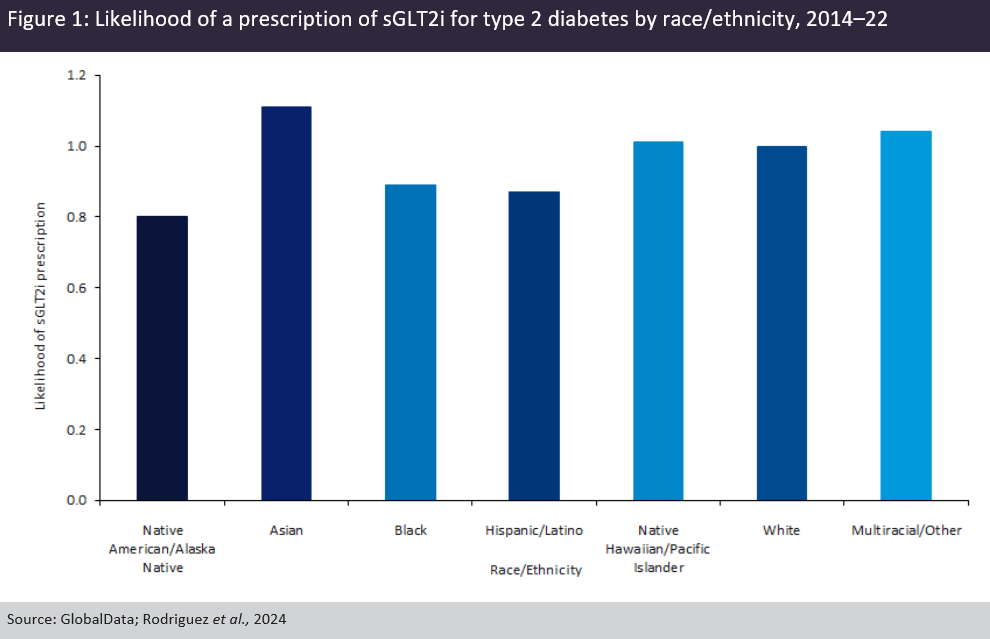
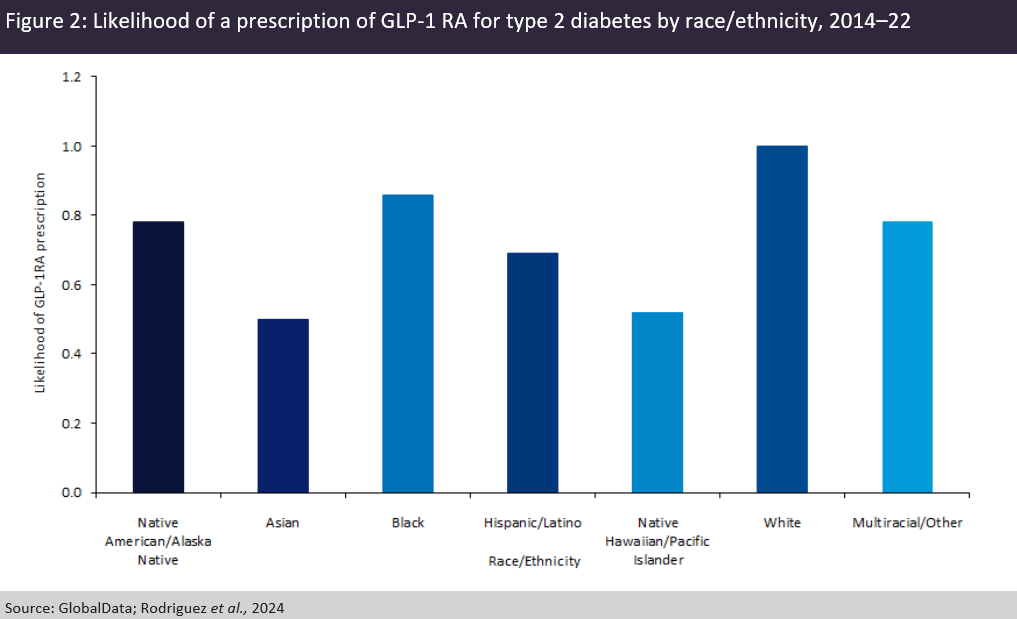
When adjusted for confounding variables, however, drug dispensation was notably unequal across racial and ethnic lines. As shown in Figure 1, Native Americans and Alaska Natives showed the lowest likelihood of receiving sGLT2is, at an odds ratio of 0.80 compared to the white reference cohort, followed by Hispanics or Latinos at 0.87 and African Americans at 0.89. Compared to their white cohorts, all racial categories showed lower odds of receiving GLP-1 RAs, with the lowest likelihood observed among Asians, Hawaiians and Pacific Islanders, and Hispanics and Latinos (Figure 2). Rodriguez and colleagues note that these results are consistent with prior scholarship, which posits that a higher occurrence of decreased healthcare access, financial barriers to care, and provider bias may lead to unequal medical care results compared to white patients.
The study carried out by Rodriguez and colleagues sheds light on the racial and ethnic inequities present in the epidemiology and treatment of diabetes in the US. Type 2 diabetes represents a growing disease burden across not only the American population, but in particularly high proportions in racial and ethnic minorities. This disease burden is exacerbated by the gaps in therapy access along similar racial lines.
More broadly, the study accentuates the paradox of race, class and American healthcare; while therapeutics have become increasingly sophisticated and effective, the management of diabetes in the US population is marred by limited access to care among disadvantaged socioeconomic classes. These contradictions present an urgent challenge to policymakers and health professionals alike to bridge the racial gap in diabetes treatment.

US Tariffs are shifting - will you react or anticipate?
Don’t let policy changes catch you off guard. Stay proactive with real-time data and expert analysis.
By GlobalData